| Outbreak: Milk Crates, Cartons, & Jugs |
|---|
| Product: Milk Crates, Cartons, & Jugs |
| Investigation Start Date: 01/27/2010 |
| Location: Roseburg, Oregon |
| Etiology: Salmonella Braenderup |
| Earliest known case onset date: 10/21/2009 |
| Latest case onset date: 10/01/2010 |
| Confirmed / Presumptive Case Counts: 25 / 0 |
| Positive Samples (Food / Environmental): 15 / 500 |
| Hospitalizations: 0 |
| Death: 0 |












| Outbreak Summary: |
|---|
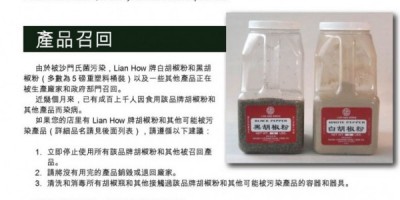
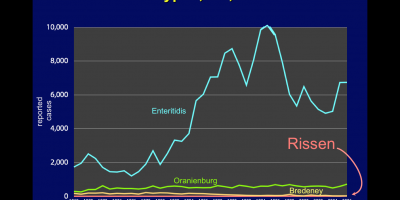
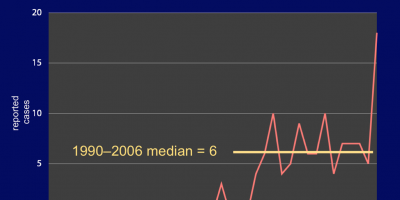
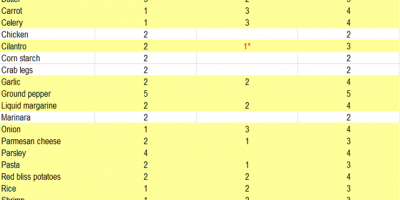
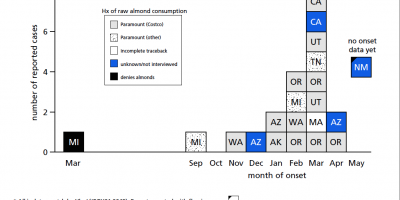
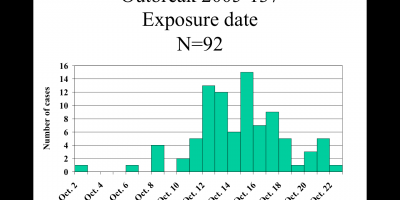
| This outbreak illustrates the value of descriptive epidemiology and the virtue of epidemiologist persistence! Over a 12-month period during 2009–2010, a total of 25 infections by Salmonella Braenderup with matching PFGE patterns were reported—no more than 4 in any given month. After 3 scattered cases over 3 months, the investigation began with recognition of a 3-case cluster in a single Oregon county in January 2010. Extensive hypothesis-generating (“shotgun”) interviews were thereafter conducted as each case was recognized, but no obvious source emerged. In desperation, on July 26, 2010, Oregon’s epidemiologists gathered to review the available information. The descriptive epidemiology proved pivotal. Person: although cases ranged in age from 1 to 88 years, there was a predilection for children: median case age was 13 years. Place: cases resided in 9 contiguous Oregon counties—but none from the populous Portland metropolitan area. Time: the prolonged duration of the outbreak ruled out most perishable items. What food or other vehicle could jibe with this information? At least 94% of cases affirmed consumption of milk—though pasteurized and of different labels. But Umpqua brand milk was known to be distributed predominantly south of the Portland area, and no other plausible hypothesis survived the analysis of the assembled epidemiologists. Experts in the Oregon Department of Agriculture were able to confirm that the alternative milk brands reported by cases or served in the case children’s schools were, in fact, produced by Umpqua. With the epidemiologists, they visited the production facility and confirmed that the pasteurization process was in order: records indicated that the milk was heated, stored, and packaged appropriately, with no apparent opportunity for post-pasteurization contamination. But culture of 132 environmental specimens obtained at the facility yielded Salmonella Braenderup in five: one from a milk crate, three from sites on the crate’s conveyor system, and one from a floor drain. The crate washer was situated on the roof of the facility, open to birds and perhaps other wildlife. The investigation tendered a surprising conclusion: the milk itself was never contaminated. Rather, the bacteria were on the milk crates, occasionally finding their way onto individual cartons, and, from perhaps one in 10,000 cartons, into someone’s mouth. This conclusion that the milk crates and cartons acted as fomites (fō’ mĭ tēz)—objects that can transfer infectious microorganisms to humans—explained the prolonged duration of the outbreak, the low attack rate, the case demographics, and the cases’ exposure histories. Finding the cause allowed for remediation and resumption of business for Umpqua: after closing for a week to sanitize and to rebuild its crate system, the plant resumed production, and the outbreak ended. |
| Details: |
|---|
| To read The Oregonian story by Lynn Terry about this outbreak, click here. INTRODUCTION: 25 cases dribbled out from Oct 2009 to Oct 2010; eventually linked to product from Umpqua Dairy in Roseburg. Crate washer was contaminating milk crates and (in turn) the sealed containers (not the milk per se). A SURPRISING TWIST: Umpqua milk products produced at the Roseburg plant have been confirmed as this source of the 25-case, year-long outbreak. In a surprising twist, however, it appears that the milk itself may NEVER have been contaminated. Rather, the weight of evidence suggested that the problem stemmed from external contamination of the milk cartons and jugs from an outdoor crate washer. In other words, the containers were fomites, meaning that by most definitions this was not a "foodborne" outbreak. Milk crates used to move product around the plant and to distribute product to retailers around the state come back to the Roseburg plant, where they recycled up a conveyor line through an outdoor crate washer and thence were carried inside the plant where they were loaded with cartons of milk. As the crates went through the washer, they were in effect being sprayed down with a solution of Salmonella Braenderup. Matching bacteria were recovered from the washer and multiple points downstream, including crates and external surfaces of sealed containers. The plant was shut for 5 days while the crate washer was disassembled, cleaned, and rebuilt, and other parts of the plant were cleaned and sanitized. Crates were boiled. New sanitizer stations were added to reduce or eliminate the risk of external contamination of the crates when they are filled with product. |